A CASE OF LABORATORY ERROR
The story:
An interesting and serious problem arose in the hospital
over the past two months.
The father of one of the children in the children's ward had had a persitent cough for the last two
weeks. He visited on a daily basis. He was reluctant to go to the local health
centre because he was busy harvesting his maize crop. He was told he must have a sputum sample
tested before he could visit again. Our senior laboratory technician was on
leave, but the junior technician said he had been trained to perform ZN
staining on a sputum sample.
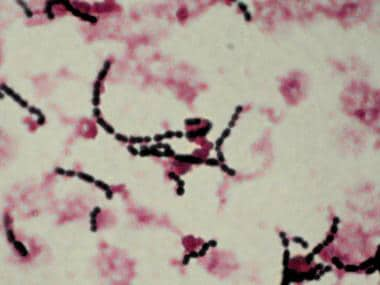
A sputum sample was obtained, and processed in the
laboratory. The technician saw the following down the microscope:

For answers to questions: See previous post: Answers to Lab Error Questions.
QUESTION 1:
This is a ZN stain of the sputum. What is seen on the slide?
The story continued:
The father had only visited his child in the ward, and had
not been close to other children. His child, who was six years old, had had a
BCG vaccination soon after birth. The father was referred to the TB clinic at
the local hospital, and told he should not visit the unit until he had been on
treatment for two weeks.
QUESTION 2:
From the above information, is it likely that any patients
or staff in the ward were at risk of aquiring TB infection from the father? If
so, give three points for action.
Five weeks later:
Five weeks after the incident, the laboratory cleaner did
not report for work for a few days. Her
daughter brought a note saying that she had a fever and a bad cough. The
previous night, the daughter said there was blood in the sputum. Four days
later, her condition worsened and she was taken to the local hospital. The
hospital laboratory examined s sputum sample and found it acid fast bacilli
positive, and a diagnosis of pulmonary tuberculosis was made. Several staff
remembered the cleaner, who also cleaned in the children's unit, had had a
cough for about a week before she took
sick leave.
QUESTION 3:
TB is not uncommon among adults in this area, so it may be
there is no link between the two cases. HOWEVER, do you have any suggestion how
there may be a link between the two cases?
A third case occurs:
Two weeks later, the laboratory aid (who is responsible for
cleaning the benches and discarding specimens) became unwell with fever and a
cough. She attended the local health centre and a sputum sample wsas sent to
the laboratory at the district hospital. It was found to be acid fast bacilli
positive.
The children's ward sister is now concerned that somehow the
ward or the laboratory was the source of infection in the cleaner and lab aid,
and an investigation is begun.
Investigating an
incident such as this has two main components:
a). To look for, and explain, epidemiological links between
the cases
b). To investigate the processing of the specimen in the laboratory.
Had the lab aid or the
cleaner come into contact with the first case?
There was no evidence that either the cleaner or the lab aid
ever came into contact with the first case. It was therefore decided to
investigate whether a breakdown in protocol had occurred in the laboratory,
resulting in infection from the sputum sample.
These were the
findings:
- the junior laboratory technician had performed ZN staining correctly and had worn a mask while handling the specimen
- the junior technician was busy with other tasks to do, and had left the specimen on the bench, rather than discarding it or putting in the refrigerator for storage
- when
the lab aid cleaned the bench the following morning, she accidently
knocked the specimen pot on the floor, which cracked and the lid fell off.
- the
cleaner, who was in the laboratory at the same time, helped the lab aid to
clean up the sputum, and rinsed the pot under a tap
QUESTION 4:
From the above findings, can you explain how and why the lab
aid and the cleaner may have become infected?
The follow up:
Following the results of the
investigation, a meeting was held with all the staff involved. The following
actions were decided:
- The
protocol for processing sputum specimens for ZN staining must be checked
to ensure correct disposal of specimens is clearly described
- The
junior technician to undergo a supervised programme with the senior
laboratory technician for all laboratory activities and demonstrate his
competence in the work
- Arrangements made for the temporary replacement of the lab aid and cleaner while they are on sick leave
- A monitoring system set up to regularly
audit the sputum processing in the laboratory
- The
clinical staff are reminded to note any children in the t who develop a
cough or fever to be referred to the paediatrician at the local hospital
- All staff told to report to a senior staff member if they develop a cough or unwell.
Both the lab aid and the cleaner made good progress on TB
treatment, and fully recovered.
This episode was a useful experience: if even a small
component of a laboratory protocol is not followed, serious infection hazards
can result.
For the Medcare programme, Uganda, the infection risk assessment proforma can be used to review the issues in this scenario.
The following link is to the form, with entries based on this case study:
Lab infection investigation form
Further reading on laboratory acquired infection:
1. TB risk among staff in a large hospital in Kenya. Int Jl TB and Lung Disease, 2008;12:949-954.
Free download at:http://www.ingentaconnect.com/content/iuatld/ijtld/2008/00000012/00000008/art00013?token=00511b8458b52781cca7b76504c48662a252c495b6c5f737b2d356a332b25757d5c4f6d4e227aaa5e
2. WHO Laboratory Bio-safety Manual.
Free download at: http://www.who.int/csr/resources/publications/biosafety/WHO_CDS_CSR_LYO_2004_11/en/
Further reading on laboratory acquired infection:
1. TB risk among staff in a large hospital in Kenya. Int Jl TB and Lung Disease, 2008;12:949-954.
Free download at:http://www.ingentaconnect.com/content/iuatld/ijtld/2008/00000012/00000008/art00013?token=00511b8458b52781cca7b76504c48662a252c495b6c5f737b2d356a332b25757d5c4f6d4e227aaa5e
2. WHO Laboratory Bio-safety Manual.
Free download at: http://www.who.int/csr/resources/publications/biosafety/WHO_CDS_CSR_LYO_2004_11/en/