An outbreak of maternal sepsis.
One week ago, JL, a 26yr old patient delivered (normal,
vaginal delivery) a healthy female child in our hospital. She was discharged to
her village the day after delivery.
Three days later a health worker came to the hospital reporting that JL was very ill, with high fever and
abdominal pain. The baby was well. We arranged for JL to be brought urgently
back to the hospital. She was admitted into a single room in the maternity
department.
QUESTIONS:
a. What do you think are
possible diagnoses?
b. What specimens would you take for the
microbiology and haematology labs?
STAGE 1:
The patient had a fever
of 40'C,
a low blood pressure, severe abdominal pain, and an odourless vaginal discharge.
While the patient was being
admitted, two things happened rather quickly: a health worker from another
village came in a hurry to the hospital and said a woman BS who had delivered
in the hospital five days ago was very ill, with symptoms sounding similar to
those of JL. Also, a nurse in the maternity ward reported that a mother AK who
had delivered two days ago, had spiked a temperature of 39'C, and had abdominal pain.
QUESTIONS:
c. What do you think is
going on?
d. Should someone assess
the baby of JL and the other patient in the village?
STAGE 2:
The following specimens
were taken on patient JL:
Blood sample for Hb and
blood count
A urine specimen for
culture and sensitivity
Blood sample for blood
culture and sensitivity
Vaginal discharge sample
for culture and sensitivity
Vaginal discharge samples
were also taken from patients BS and AK.
LABORATORY RESULTS:
1. Hb 9.6 g/dl. White cell
count 22,000, 90% polymorphs.
2. The findings in the
microbiology lab are shown below:
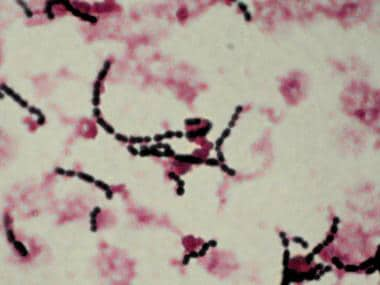
Microscopy of the vaginal
discharge: Culture appearance of vaginal discharge
(Gram
stain) on
blood agar

QUESTIONS:
e. Describe the Gram stain
and the culture appearances
f. What is the possible
bacteria causing the discharge, and the infection?
THE STORY CONTINUES:
There are three patients
with the same infection, all apparently originating from the maternity unit.
This suggests a small outbreak, and cross infection. As well as diagnosing the individual patients,
we need to investigate the outbreak, and hopefully stop further infections.
INVESTIGATING AND CONTROLLING THE OUTBREAK :
(Remember Semmelweis,
1847. ..Google this if you are not sure).
While post partum sepsis
may arise from bacteria the mother was carrying, as there are three linked
cases, it suggests infection is being transmitted between patients, or from a
common source; how might this happen?
We need to look at the
practices and other factors associated with the maternity ward. These are some of the questions to ask:
1. Is common equipment
used between patients, eg a speculum?, how is it cleaned between patients?
2. Were the three cases in
the ward at the same time.
3. Do delivery
nurses/midwives wear gloves for examinations and deliveries? are these gloves
changed between patients?
4. Are the hand washing
facilities on the ward adequate? are water and soap always available?
5. Is the general hygiene
of the ward (floors, bed sheets, patient washing etc) adequate.
FINDINGS:
a. All three mothers had been in the same ward
for at least one day together, JL and BS post delivery, and AK the day before
delivery
b. Nurses were certain
that they changed gloves between patients, but observation showed that when the
ward was very busy and several mothers ready to deliver at the same time, this
did not always happen
c. There were only three
specula on the unit, but they seemed to be cleaned appropriately between
patient use
d. The general hygiene on
the ward seemed to be adequate although resources were limited.
e. Although there were
sinks and soap , hand washing practices could have been improved:
INTERPRETING THE FINDINGS:
The cause of the infections
was Streptococcus pyogenes, Group A Strep.
This is a Gram positive
coccus, appearing in chains, and producing beta (clear) haemolysis on culture
on blood agar.
Fortunately Gp A streps
remain sensitive to penicillin.
It is probable that one
patient was colonised vaginally with Gp A strep, and this was transmitted to
the other two patients by the unchanged gloves of one of the staff.
LESSONS:
a. Maternal (puerperal)
sepsis is not uncommon in low resource areas, is potentially fatal, but can
respond to penicillin if treated early
b. While the lab diagnosis
was not essential for managing the individual patients (though it did confirm the
diagnosis), it was essential to show that cross infection had occurred.
c. In district hospitals
in 2015, wherever they are located, microbiology labs should be able to do
culture and sensitivity
d. If there appears to be
a cluster of infections, or an outbreak, some basic epidemiology related
questions must be asked: who is affected, where were they, when did they become
ill, what factors may have caused transmission, are basic infection control
measures adequate?
e. Based on the above,
changes must be implemented to improve infection prevention and control
Link to Tropical Microbiology Laboratory website for more details on lab methods:
https://sites.google.com/site/tropmicrolaboratorynetwork/
Further reading on maternal sepsis:
https://sites.google.com/site/tropmicrolaboratorynetwork/
Further reading on maternal sepsis:
1. Maternal and early onset neonatal bacterial sepsis:
burden and
strategies for prevention in sub-Saharan Africa .
Lancet infectious diseases 2009; 9: 428-438.
2. Microbial profile in women with puerperal sepsis in Gadarif State ,
Eastern Sudan
Annals of
Tropical Medicine and Public Health, 2013;6: 460-464.