Tuesday, 15 March 2016
MICROBIOLOGY BLOG FOR YOUR DISTRICT
CREATE YOUR OWN MICROBIOLOGY BLOG IN YOUR DISTRICT
The Zura Health Programme microbiology blog is an example of how microbiology and infection news can be shared between labs and hospitals in a district or region.
The different posts can be accessed from the sidebar on the right.
A blog can be used to keep colleagues aware of new infection problems, to update them on information, and as a contribution to continuing education and professional development.
If your hospital has internet access, creating and maintaining a blog is easy.
The two most convenient ways of creating a blog are in Google:
https://support.google.com/blogger/answer/1623800?hl=en
or Wordpress:
https://wordpress.com/learn-more/?v=blog
We hope you have found this blog interesting, and an encouragement to develop a microbiology/blog in your district. Just think how such a set up could have helped in the 2014/5 Ebola outbreak, to have a network of communication and support between distant hospitals.
If you have ideas for new posts, or want to discuss ideas for a blog in your area, put some comments at the bottom of the post pages.
Namaste
Ma'a Salaama
Kwaheri
Thursday, 10 March 2016
USING MAPS IN A TB CONTROL PROGRAMME
Multi Drug Resistant
Tuberculosis: Creating maps to help the control programme.


During the last month, there were 30 new cases of TB
diagnosed (by ZN microscopy) in the laboratory. The samples were from three
health centre in Zura district. 10 of the samples were sent to the national TB
laboratory for sensitivity testing, and of these, six were MDRTB. Four were
from one HC and two from an adjacent HC area. Three months earlier, there had
been four cases of MDRTB from one of these areas.
Although TB is endemic in our area (despite the national TB
programme), these were the first cases of MDRTB that had occurred. We thought
it was time to get a clearer understanding of the pattern of TB in the
district, and to look back on all the cases we had had over the last year. We
hoped that this may help to improve control locally, and ensure that best use
was being made of the laboratory for TB in the community, as well as for
individual new cases.
Our plan was to do two things:
a): on a spreadsheet eg Excel, list all the cases, with date
of diagnosis, age, village, local HC, if they were MDRTB, if after 4 months
they were still taking regular treatment.
b): put the information on a map, so that possible links
between cases could be seen, possible clusters
of MDRTB identified, and village health workers could easily see the location
of cases in their areas.
For mapping, there are several possibilities. If your region has access to the WHO
Healthmapper for your country, this may be the best system to use, but
availability and permission for you to make local maps would depend on the MoH.
Free software such as EPI-Map (from the CDC website) is useful, but not
particularly flexible for unskilled users. Professional mapping systems such as
ARC-Info make the most sophisticated maps, but are expensive and complicated.
If your hospital/lab has internet access, then Google maps
provides a useful and simple way of creating maps for local health programmes.
You need to have a Google account (eg Gmail). Creating your own maps in Google maps requires
some persistence and trial and error, but once you are used to it, they are
easy to create.
Examples of maps we created and used are shown below:

The view above shows the boundaries of the sub-districts,
the location of the health centres, and the location of each of the TB cases,
and whether or not they are MDRTB.
The second view (below) is in "satellite" mode,
and zoomed in to show the detailed location of cases in their village areas.
Such a view can help very much in seeing links between cases, and in contact
tracing.

The third view(below) again shows the location of individual
cases, and in addition the data table that is automatically created in Google
maps as each new point is added. It also shows the pop-up box for a case that
is highlighted, so that the details on each case can easily be seen.

A Google map is an online map, not a static map on your
computer. This means several things:
- You can share the map in real time with others on the internet to whom you have given the link (eg the district TB office, health workers if they have internet access on computer or smart phone, other hospitals if there are cases between districts),
- The map can be updated each time there is a new case, without having to create a new map
- You can zoom in and out of the map, to see the overall cases or concentrate on one area to see case location, and you can alternate between map and satellite view
- The map can be printed off, so that health centres without internet access can have a weekly updated map supplied
In our programme, we used the maps we created for the
following ways to assist the TB control programme.
1. Looking at the overall geographical spread of TB cases in
the project area to see if there are particular areas of clusters/high
transmission.
2. To look at the location of MDRTB cases. Are they sporadic or are they in clusters. Do
they occur mainly in one area of the project? (eg a village where many men go
as migrant workers to an industrial area).
3. Contact tracing. We can draw a eg 500m zone around a new
case, on satellite view zoom in and see actual houses nearby, and arrange and
mark off contact tracing.
4. As soon as a new case is diagnosed in the lab, it can be
added to the map, and immediately seen by any health worker accessing the map.
It can be colour coded according to normal case or MDRTB. With the "pop
up" box for the new case, details such as age, village, date of diagnosis
can readily be seen.
5. The case load for each HCW can easily be seen from the
number of cases in their block.
6. The data table
generated in the map as each new case is added can easily be visualised to show
the cases in tabular form.
7. Weekly or monthly maps, using whichever view required,
can be printed off for hard copy reports, or distributed to HC's without
computers/internet access.
8. Maps can be saved to a file on the computer.
We have found that using such a web based and shared map
helps us to be more aware of the pattern of TB cases, and helps in the day to
day running of the programme.
Further reading on disease mapping:
1. Identification of malaria hotspots in a tribal area of India. Int J Health Geog,2009;8 (This is rather complicated, but similar work could be done with Google maps).
https://ij-healthgeographics.biomedcentral.com/articles/10.1186/1476-072X-8-30
2. Mapping TB in Malawi. Malawi Med J 2005;17:33-35.
https://www.researchgate.net/publication/269103003_Not_just_pretty_pictures_Geographical_Information_Systems_in_TB_control
Two other useful sites for disease outbreak maps and lists are:
Healthmap:
http://www.healthmap.org/en/
ProMedmail:
http://www.promedmail.org/
Further reading on disease mapping:
1. Identification of malaria hotspots in a tribal area of India. Int J Health Geog,2009;8 (This is rather complicated, but similar work could be done with Google maps).
https://ij-healthgeographics.biomedcentral.com/articles/10.1186/1476-072X-8-30
2. Mapping TB in Malawi. Malawi Med J 2005;17:33-35.
https://www.researchgate.net/publication/269103003_Not_just_pretty_pictures_Geographical_Information_Systems_in_TB_control
Two other useful sites for disease outbreak maps and lists are:
Healthmap:
http://www.healthmap.org/en/
ProMedmail:
http://www.promedmail.org/
Friday, 19 February 2016
ANTIMICROBIAL RESISTANCE
A POST ON
ANTIMICROBIAL RESISTANCE

Global
microbiology arrived in our small laboratory last week with the isolation of a Klebsiella pneumoniae, that appeared to
be resistant to all antibiotics. It was from the sputum of a post operative
patient, who had been in the hospital for two weeks.
Below is a photo of the disc sensitivity plate:






Below is a photo of the disc sensitivity plate:

What
does this finding mean for a small rural hospital laboratory, and how did we
deal with it ?
To
begin with, it may be useful to have an
update on how increasing antibiotic resistance in Gram negative bacteria such
as E.coli and Klebsiella spp has evolved over the last 10 years, and to
understand some of the terms such as ESBL, Carbapenemase producers, metallobeta-lactamases, VIM and NDM-1, terms you may have seen if you
have seen in recent microbiology/infection journals.
Some readers of the post will
know all of this, but there may be some who have not had the opportunity to
keep up to date. So this discussion is mostly for the latter readers.
You will remember that beta
lactamases are enzymes produced by many bacteria, that break down the structure
of penicillin and similar antibiotics, so that the antibiotic can no longer
kill the bacteria. Extended spectrum beta lactamases (ESBL's) are, as it says,
beta lactamases with a spectrum of activity against a wider range of penicillin
and cephalosporin antibiotics, so limiting the treatment options for infections
caused by ESBL producing bacteria.
In the disc sensitivity
testing, an E.coli or Klebsiella that has no zone to a third generation
cephalosporin (cefotaxime, ceftazidime, cefixime etc), should be considered as
an ESBL producer. A further test is required to determine if it definitely is
an ESBL producer, one commonly used is the double disc test:
Method:
The double disc method compares the zone sizes of the
isolate around a cefotaxime disc, and a combined cefotaxime plus clavulanic
acid disc. A greater than 5mm diference between the zone size around the combined
disc (the larger zone) and the cefotaxime disc confirms ESBL production.
The slide below shows a positive ESBL result.

While some rural hospital
laboratories may be able to set this up, it may be better that the regional
hospital has this facility, and smaller laboratories send suspected ESBL
isolates to the regional laboratory.
When considering antimicrobial
resistance, two components need to be
considered:
a) the mechanism of
resistance, eg a drug destroying enzyme such as a beta lactamase, the blocking
of antibiotic uptake (tetracycline resistance), producing an alternative
metabolic pathway (trimethoprim resistance)
b) the bacterial genes that
code for the resistance mechanism, and how they are acquired by a bacteria.
One of the primary reasons
why antibiotic resistance spreads both locally and regionally is that in many
cases the genes coding for a resistance mechanism can be transferred between
bacteria, and often a group of genes, coding for several resistance mechanisms,
can be transferred together.
This is why we may see an
E.coli that is an ESBL producer, and therefore resistant to penicillins and
cephalosporins, and also resistant to aminoglycosides (gentamicin, amikacin),
and to fluoroquinolones such as ciprofloxacin.
If such an E.coli was
isolated from a blood culture, or a urinary tract infection, the options for
treatment are very limited, and this is what is increasingly happening, even in
rural tropical areas. In many places,
there would be no further antibiotic available, making treatment impossible.
The main group of antibiotics
that can be used to treat such infections are the carbapenems, of which
imipenem and meropenem are the main examples. Where these drugs are available,
particularly in hospitals, they have been used to treat these highly resistant
Gram negative infections.
However, a few years back,
E.coli and Klebsiella strains were isolated that had also become resistant to
carbapenems in addition to the other antibiotics. Investigations showed that
they produced an enzyme, similar to beta lactamase called a carbapenemase,
which inactivated the carbapenem antibiotic.
Below
is a sensitivity plate with a Klebsiella pneumoniae resistant to imipenem and
meropenem:

These new beta lactamases
were found to have a metal ion in their molecule, and were called
metallo-beta-lactamases. One of the first ones isolated and investigated was in
New Delhi, India, and was labelled as New Delhi metallo-beta-lactamase-1, or
NDM-1, a term you may have seen. Other metallo-beta-lactamases have been
described, with names including VIM and OXA-48.
As with other resistance
mechanisms, these are coded for by specific genes, which can move between
bacteria. Therefore, an E.coli, which is an ESBL producer and resistant also to
gentamicin and ciprofloxacin, could acquire the gene for NDM-1, and be resistant
also to meropenem.
As with ESBL's, while the
initial disc testing with resistance to meropenem/imipenem suggests a probable
carbapenemase producer, further testing is required to confirm this. A special
disc test (the Hodge test) can be used, but this is difficult to set up and
monitor, and would more accurately be done at a regional laboratory.
Specialised laboratories now use molecular tests (which we will talk about in
post 11) to detect specific carbapenemase genes such as NDM-1.
Well, that's the end of the
lecture !

So back to the question, if
you start isolating resistant bacteria, whether ESBL producers or worse, what
should the laboratory, and the hospital do about it?
Here is our experience.
The isolation of this
multi-resistant Klebsiella made us realise that we didn't actually know how
many times in the past we had isolated bacteria with resistance to most of our
commonly available antibiotics, even if not as multi-resistant as this one.
While we kept a day book of which bacteria had been isolated from which
specimen (and date, patient details, etc) we had not been recording the
sensitivity profile.
So, this was the first
action. To begin a new day book (either an actual register, or on a spreadsheet
on the computer), with columns in which to put sensitivity or resistance to the
antibiotics tested. We in fact decided to have both a day book register, which
the lab staff are used to using, but, as we had a computer with Excel on it,
also to set up a spreadsheet. The spreadsheet is updated from the day book at the end of
each day. The advantage of the spreadsheet is that each month we can easily
analyse how many isolates have been resistant to different antibiotics, how
many are multi resistant. Also we can produce graphs and charts that we can use
in a presentation to the doctors for them to be aware of the problem of
antibiotic resistance. More details of setting up spreadsheets and databases to
monitor infections will be given in post 9.
The second action was to be
sure that our sensitivity testing was in fact accurate. We use the CSLI disc
diffusion method. From a survey that was done in laboratories in district
hospitals in our region last year, including sending round some test samples
for comparison, it was evident that different laboratories were getting
different results for the same isolate , and not all were following the correct
criteria for the CLSI method that they said they were using.
One of the main problems was
that rather than accurately measuring the zone diameter of "no growth"
around a disc and comparing this to the standard table, laboratory staff were
just comparing by eye zone sizes, writing down a "large" zone as
"sensitive" and a small zone sometimes as "resistant" and
sometimes as "partially sensitive".
This is illustrated in the
image below:

We decided to look carefully
at the CLSI protocol (ref link ) to ensure we were doing sensitivity testing
correctly. You can check the link to assess your methods. The most important
points to follow we realised are:
- Have some control organisms from the regional
laboratory (E.coli, S.aureus, Pseudomonas aeruginosa), and do disc
sensitivity with these and check against the CLSI control table that the
zone sizes for different antibiotic discs with these control organisms are
correct. This ensures that our stock of discs are potent, and our culture
conditions are correct
- When testing clinical isolates, compare the zone
sizes with the CLSI clinical samples table, and decide whether isolates
are sensitive or resistant based on these sizes, not just by looking at
the zone size.
A detailed description of the CLSI method is available
at the following website:
http://www.microbelibrary.org/component/resource/laboratory-test/3189-kirby-bauer-disk-diffusion-susceptibility-test-protocol
An example of cut-off zone
sizes for a range of antibiotics is given in the table below:

This has been a rather long post! but it is
an important topic, we have had to learn new things, and we hope it has been
useful to you.
Further reading on Antimicrobial Resistance:
1. Increased multi-drug resistant E.coli from hospitals in Khartoum State, Sudan. Afr Health Sci 2012; 12:368-375.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3557680/
2. WHO global report on antimicrobial resistance and surveillance.
http://www.who.int/drugresistance/documents/surveillancereport/en/
Further reading on Antimicrobial Resistance:
1. Increased multi-drug resistant E.coli from hospitals in Khartoum State, Sudan. Afr Health Sci 2012; 12:368-375.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3557680/
2. WHO global report on antimicrobial resistance and surveillance.
http://www.who.int/drugresistance/documents/surveillancereport/en/
Friday, 11 December 2015
A LABORATORY ERROR
A CASE OF LABORATORY ERROR
The story:
An interesting and serious problem arose in the hospital
over the past two months.
The father of one of the children in the children's ward had had a persitent cough for the last two
weeks. He visited on a daily basis. He was reluctant to go to the local health
centre because he was busy harvesting his maize crop. He was told he must have a sputum sample
tested before he could visit again. Our senior laboratory technician was on
leave, but the junior technician said he had been trained to perform ZN
staining on a sputum sample.
A sputum sample was obtained, and processed in the
laboratory. The technician saw the following down the microscope:

For answers to questions: See previous post: Answers to Lab Error Questions.
QUESTION 1:
This is a ZN stain of the sputum. What is seen on the slide?
The story continued:
The father had only visited his child in the ward, and had
not been close to other children. His child, who was six years old, had had a
BCG vaccination soon after birth. The father was referred to the TB clinic at
the local hospital, and told he should not visit the unit until he had been on
treatment for two weeks.
QUESTION 2:
From the above information, is it likely that any patients
or staff in the ward were at risk of aquiring TB infection from the father? If
so, give three points for action.
Five weeks later:
Five weeks after the incident, the laboratory cleaner did
not report for work for a few days. Her
daughter brought a note saying that she had a fever and a bad cough. The
previous night, the daughter said there was blood in the sputum. Four days
later, her condition worsened and she was taken to the local hospital. The
hospital laboratory examined s sputum sample and found it acid fast bacilli
positive, and a diagnosis of pulmonary tuberculosis was made. Several staff
remembered the cleaner, who also cleaned in the children's unit, had had a
cough for about a week before she took
sick leave.
QUESTION 3:
TB is not uncommon among adults in this area, so it may be
there is no link between the two cases. HOWEVER, do you have any suggestion how
there may be a link between the two cases?
A third case occurs:
Two weeks later, the laboratory aid (who is responsible for
cleaning the benches and discarding specimens) became unwell with fever and a
cough. She attended the local health centre and a sputum sample wsas sent to
the laboratory at the district hospital. It was found to be acid fast bacilli
positive.
The children's ward sister is now concerned that somehow the
ward or the laboratory was the source of infection in the cleaner and lab aid,
and an investigation is begun.
Investigating an
incident such as this has two main components:
a). To look for, and explain, epidemiological links between
the cases
b). To investigate the processing of the specimen in the laboratory.
Had the lab aid or the
cleaner come into contact with the first case?
There was no evidence that either the cleaner or the lab aid
ever came into contact with the first case. It was therefore decided to
investigate whether a breakdown in protocol had occurred in the laboratory,
resulting in infection from the sputum sample.
These were the
findings:
- the junior laboratory technician had performed ZN staining correctly and had worn a mask while handling the specimen
- the junior technician was busy with other tasks to do, and had left the specimen on the bench, rather than discarding it or putting in the refrigerator for storage
- when
the lab aid cleaned the bench the following morning, she accidently
knocked the specimen pot on the floor, which cracked and the lid fell off.
- the
cleaner, who was in the laboratory at the same time, helped the lab aid to
clean up the sputum, and rinsed the pot under a tap
QUESTION 4:
From the above findings, can you explain how and why the lab
aid and the cleaner may have become infected?
The follow up:
Following the results of the
investigation, a meeting was held with all the staff involved. The following
actions were decided:
- The
protocol for processing sputum specimens for ZN staining must be checked
to ensure correct disposal of specimens is clearly described
- The
junior technician to undergo a supervised programme with the senior
laboratory technician for all laboratory activities and demonstrate his
competence in the work
- Arrangements made for the temporary replacement of the lab aid and cleaner while they are on sick leave
- A monitoring system set up to regularly
audit the sputum processing in the laboratory
- The
clinical staff are reminded to note any children in the t who develop a
cough or fever to be referred to the paediatrician at the local hospital
- All staff told to report to a senior staff member if they develop a cough or unwell.
Both the lab aid and the cleaner made good progress on TB
treatment, and fully recovered.
This episode was a useful experience: if even a small
component of a laboratory protocol is not followed, serious infection hazards
can result.
For the Medcare programme, Uganda, the infection risk assessment proforma can be used to review the issues in this scenario.
The following link is to the form, with entries based on this case study:
Lab infection investigation form
Further reading on laboratory acquired infection:
1. TB risk among staff in a large hospital in Kenya. Int Jl TB and Lung Disease, 2008;12:949-954.
Free download at:http://www.ingentaconnect.com/content/iuatld/ijtld/2008/00000012/00000008/art00013?token=00511b8458b52781cca7b76504c48662a252c495b6c5f737b2d356a332b25757d5c4f6d4e227aaa5e
2. WHO Laboratory Bio-safety Manual.
Free download at: http://www.who.int/csr/resources/publications/biosafety/WHO_CDS_CSR_LYO_2004_11/en/
Further reading on laboratory acquired infection:
1. TB risk among staff in a large hospital in Kenya. Int Jl TB and Lung Disease, 2008;12:949-954.
Free download at:http://www.ingentaconnect.com/content/iuatld/ijtld/2008/00000012/00000008/art00013?token=00511b8458b52781cca7b76504c48662a252c495b6c5f737b2d356a332b25757d5c4f6d4e227aaa5e
2. WHO Laboratory Bio-safety Manual.
Free download at: http://www.who.int/csr/resources/publications/biosafety/WHO_CDS_CSR_LYO_2004_11/en/
ANSWERS TO LAB ERROR QUESTIONS
ANSWERS TO THE
QUESTIONS ON THE LABORATORY ERROR POST
QUESTION 1:
This is a ZN stain of
the sputum. What is seen on the slide?
Pink bacilli (rod shaped bacteria), these are acid fast
bacilli, typical of mycobacteria. While the sputum would have to be cultured to
confirm the diagnosis, it is probably Mycobacterium tuberculosis.
QUESTION 2:
From the above
information, is it likely that any patients or staff in the ward were at risk
of acquiring TB infection from the father? If so, give three points for action.
The father is sputum positive, that means he is infectious
with TB, and could infect anyone (patients or staff) who is susceptible, and
who was close to him when he was coughing.
Action points could include the following:
§
Check if any children on the ward had not had
BCG. Advice from the district TB officer should be sought. This would be
particularly important if any child was known to be HIV positive, or had other
reason for reduced immunity
§
All staff should be told to inform the senior
hospital nurse if they develop a cough or become otherwise unwell
§
QUESTION 3:
TB is not uncommon
among adults in this area, so it may be there is no link between the two cases.
HOWEVER, do you have any suggestion how there may be a link between the two cases?
The possible links (but we do not know the answers yet)
could be:
a). The lab aid and the cleaner were both on the children's
ward at various times when the father was there, and so became infected from
him,
b). There may be no link, either with the father or the
hospital. Both could have been infected in the community,
c). They may both have been exposed to infection in the
laboratory.
QUESTION 4:
From the findings, can
you explain how and why the lab aid and the cleaner may have become infected,
but not the junior technician?
(These were the
findings:
- the junior laboratory technician had
performed ZN staining correctly and had worn a mask while handling the
specimen
- the junior technician was busy with
other tasks to do, and had left the specimen on the bench, rather than
discarding it or putting in the refrigerator for storage
- when the lab aid cleaned the bench the
following morning, she accidently knocked the specimen pot on the floor,
which cracked and the lid fell off.
- the cleaner, who was in the laboratory
at the same time, helped the lab aid to clean up the sputum, and rinsed
the pot under a tap)
The junior technician wore a mask while processing the
specimen, and apart from not discarding the specimen correctly, appears to have
followed the correct protocol.
Both the lab aid and the cleaner were exposed to infectious
material when the specimen pot fell and cracked, and in the process of cleaning
up.
Friday, 20 November 2015
AN OUTBREAK OF MATERNAL SEPSIS
An outbreak of maternal sepsis.
One week ago, JL, a 26yr old patient delivered (normal,
vaginal delivery) a healthy female child in our hospital. She was discharged to
her village the day after delivery.
Three days later a health worker came to the hospital reporting that JL was very ill, with high fever and
abdominal pain. The baby was well. We arranged for JL to be brought urgently
back to the hospital. She was admitted into a single room in the maternity
department.
QUESTIONS:
a. What do you think are
possible diagnoses?
b. What specimens would you take for the
microbiology and haematology labs?
STAGE 1:
The patient had a fever
of 40'C,
a low blood pressure, severe abdominal pain, and an odourless vaginal discharge.
While the patient was being
admitted, two things happened rather quickly: a health worker from another
village came in a hurry to the hospital and said a woman BS who had delivered
in the hospital five days ago was very ill, with symptoms sounding similar to
those of JL. Also, a nurse in the maternity ward reported that a mother AK who
had delivered two days ago, had spiked a temperature of 39'C, and had abdominal pain.
QUESTIONS:
c. What do you think is
going on?
d. Should someone assess
the baby of JL and the other patient in the village?
STAGE 2:
The following specimens
were taken on patient JL:
Blood sample for Hb and
blood count
A urine specimen for
culture and sensitivity
Blood sample for blood
culture and sensitivity
Vaginal discharge sample
for culture and sensitivity
Vaginal discharge samples
were also taken from patients BS and AK.
LABORATORY RESULTS:
1. Hb 9.6 g/dl. White cell
count 22,000, 90% polymorphs.
2. The findings in the
microbiology lab are shown below:
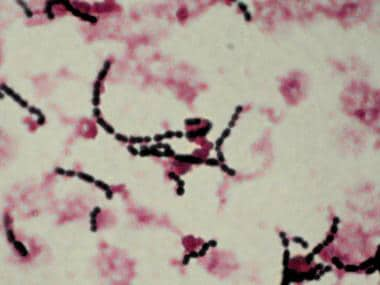
Microscopy of the vaginal
discharge: Culture appearance of vaginal discharge
(Gram
stain) on
blood agar

QUESTIONS:
e. Describe the Gram stain
and the culture appearances
f. What is the possible
bacteria causing the discharge, and the infection?
THE STORY CONTINUES:
There are three patients
with the same infection, all apparently originating from the maternity unit.
This suggests a small outbreak, and cross infection. As well as diagnosing the individual patients,
we need to investigate the outbreak, and hopefully stop further infections.
INVESTIGATING AND CONTROLLING THE OUTBREAK :
(Remember Semmelweis,
1847. ..Google this if you are not sure).
While post partum sepsis
may arise from bacteria the mother was carrying, as there are three linked
cases, it suggests infection is being transmitted between patients, or from a
common source; how might this happen?
We need to look at the
practices and other factors associated with the maternity ward. These are some of the questions to ask:
1. Is common equipment
used between patients, eg a speculum?, how is it cleaned between patients?
2. Were the three cases in
the ward at the same time.
3. Do delivery
nurses/midwives wear gloves for examinations and deliveries? are these gloves
changed between patients?
4. Are the hand washing
facilities on the ward adequate? are water and soap always available?
5. Is the general hygiene
of the ward (floors, bed sheets, patient washing etc) adequate.
FINDINGS:
a. All three mothers had been in the same ward
for at least one day together, JL and BS post delivery, and AK the day before
delivery
b. Nurses were certain
that they changed gloves between patients, but observation showed that when the
ward was very busy and several mothers ready to deliver at the same time, this
did not always happen
c. There were only three
specula on the unit, but they seemed to be cleaned appropriately between
patient use
d. The general hygiene on
the ward seemed to be adequate although resources were limited.
e. Although there were
sinks and soap , hand washing practices could have been improved:
INTERPRETING THE FINDINGS:
The cause of the infections
was Streptococcus pyogenes, Group A Strep.
This is a Gram positive
coccus, appearing in chains, and producing beta (clear) haemolysis on culture
on blood agar.
Fortunately Gp A streps
remain sensitive to penicillin.
It is probable that one
patient was colonised vaginally with Gp A strep, and this was transmitted to
the other two patients by the unchanged gloves of one of the staff.
LESSONS:
a. Maternal (puerperal)
sepsis is not uncommon in low resource areas, is potentially fatal, but can
respond to penicillin if treated early
b. While the lab diagnosis
was not essential for managing the individual patients (though it did confirm the
diagnosis), it was essential to show that cross infection had occurred.
c. In district hospitals
in 2015, wherever they are located, microbiology labs should be able to do
culture and sensitivity
d. If there appears to be
a cluster of infections, or an outbreak, some basic epidemiology related
questions must be asked: who is affected, where were they, when did they become
ill, what factors may have caused transmission, are basic infection control
measures adequate?
e. Based on the above,
changes must be implemented to improve infection prevention and control
Link to Tropical Microbiology Laboratory website for more details on lab methods:
https://sites.google.com/site/tropmicrolaboratorynetwork/
Further reading on maternal sepsis:
https://sites.google.com/site/tropmicrolaboratorynetwork/
Further reading on maternal sepsis:
1. Maternal and early onset neonatal bacterial sepsis:
burden and
strategies for prevention in sub-Saharan Africa .
Lancet infectious diseases 2009; 9: 428-438.
2. Microbial profile in women with puerperal sepsis in Gadarif State ,
Eastern Sudan
Annals of
Tropical Medicine and Public Health, 2013;6: 460-464.
Subscribe to:
Comments (Atom)